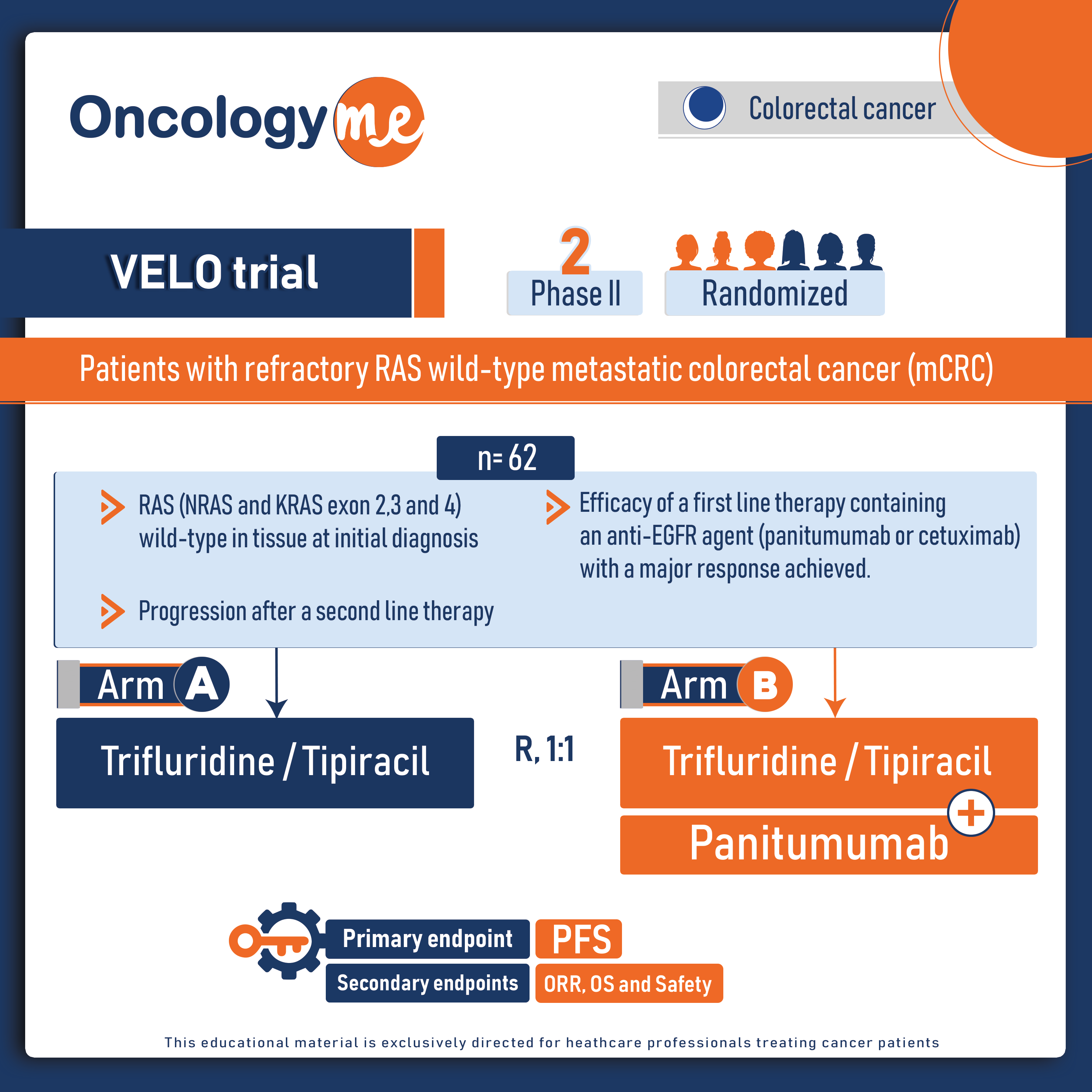
In the randomized, phase II VELO trial, third-line treatment with the anti-EGFR monoclonal antibody #panitumumab plus the standard-of-care trifluridine-tipiracil significantly improved progression-free survival (PFS) for patients with refractory RAS wild-type metastatic colorectal cancer (#mCRC).
The study included 62 chemo-refractory RAS wild-type mCRC patients who had previously responded well to first-line chemotherapy plus an anti-EGFR monoclonal antibody and had a four-month or longer anti-EGFR drug-free interval during second-line therapy. These patients were randomly assigned to receive either trifluridine-tipiracil alone (Arm A) or trifluridine-tipiracil plus panitumumab (Arm B). Baseline plasma was analyzed for circulating free tumor (ct) DNA to detect mutations in KRAS, NRAS, BRAF (V600E) and EGFRextracellular domain (S492R). Moreover, liquid biopsy using FoundationOne Liquid CDx (324 gene profiling) was conducted to detect mutations in KRAS, NRAS, BRAF (V600E), and EGFR extracellular domain (S492R) in 24 patients with baseline RAS/BRAF wild-type circulating free tumor (ct) DNA, both before treatment and at disease progression.
The primary endpoint was progression free survival (PFS), secondary end points included overall survival (OS). The primary endpoint of improved PFS was met, with a median PFS of 4 months in Arm B compared to 2.5 months in Arm A (HR=0.48, p = 0.007). Among patients with baseline RAS/BRAF wild-type ctDNA, the median PFS was even better with adding panitumumab (4.5 ms versus 2.6 ms, HR=0.48, p = 0.019). Disease control, defined as major responses plus stable disease, was higher in patients receiving trifluridine-tipiracil plus panitumumab (81%) compared to those receiving trifluridine-tipiracil alone (48%). Median OS was 13.1 months in Arm A and 11.6 months in Arm B, but this difference was not statistically significant (HR: 0.96, p = 0.9).
To assess the impact of subsequent lines of treatment on survival, researchers performed subgroup analysis on the 24 out of 30 patients in Arm A who received fourth-line therapy after progression on trifluridine/tipiracil. Of these patients, 17 were rechallenged with anti-EGFR therapies, while 7 received regorafenib. The median PFS was 4.1 months for patients treated with anti-EGFR rechallenge therapy compared to 3.0 months for regorafenib treatment (HR: 0.29, p = 0.024). Seven out of 17 patients treated with anti-EGFR rechallenge therapy experienced prolonged PFS (>6 months). Median OS from the start of fourth-line treatment was 13.6 months for patients treated with anti-EGFR rechallenge therapy and 5.1 months for those treated with regorafenib (HR: 0.30, p = 0.019).
Overall, the Velo trial represents the first prospective randomized study evaluating the addition of the anti-EGFR monoclonal antibody panitumumab to the standard-of-care trifluridine-tipiracil as third-line rechallenge therapy in chemo-refractory RAS wild-type mCRC patients. While this was a phase II study with its limitations, the final results provide clinical evidence supporting the efficacy of anti-EGFR rechallenge as a treatment option for patients with RAS wild-type refractory mCRC, both as a third-line and a fourth-line therapy.
.png)